

Active Suicidal Ideation vs. Passive Suicidal Ideation
Suicidal ideation (thoughts of suicide) can feel like a very big topic, and it may not have been something your family or community discussed. Suicide and suicidal ideation have carried stigma for a long time. A significant part of this stigma was due to the criminalization of suicide in many places. If someone was “found guilty” of making a suicide attempt or “committing” suicide, the consequences (depending on the place and time) could have involved fines, jail time, confiscation of property, disrespectful burials, or prohibition of a funeral. Suicide has been decriminalized, which is an important reason to shift your language from “committed suicide” to “died by suicide.”
This blog will help break down the components of suicidal ideation and the difference between active and passive suicidal ideation.
There are several different components of suicidal ideation.
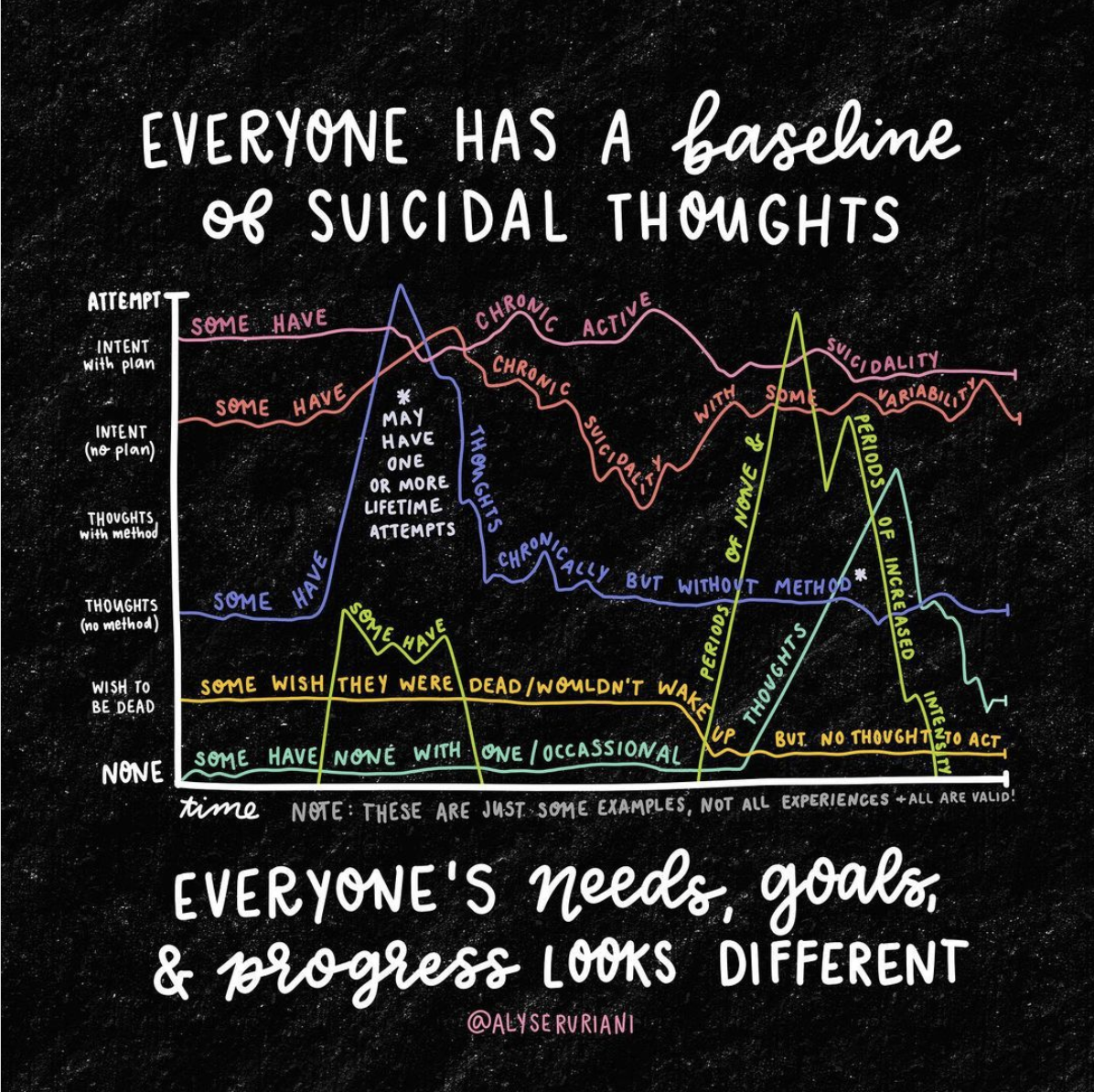
Suicidal Ideation components
Thoughts: Are you having thoughts about suicide? Are you having thoughts of not wanting to be alive?
Plan: Do you have a plan of how you would kill yourself?
Means: What would you use to kill yourself? Do you have access
Intent: Are you thinking about following through with your plan?
Time Frame: Do you have a time frame of when you are thinking about following through with your plan?
Severity: How intense or severe are these thoughts?
If you aren’t used to having conversations about suicide, these questions might feel abrasive or overly direct. It makes sense that you may feel a little uncomfortable with these questions at first, but it is helpful to be direct when talking about suicide. Using direct language when talking about suicide communicates to the other person that you are not afraid of their suicidal ideation and that you are showing up to support them. Breaking down suicidal ideation into the components listed above also helps provide support and specific coping skills. Your therapist will assess these different components so that they know how to support you and use an appropriate intervention level. Hopefully, your therapist’s goal is to respond to your active SI with the least invasive intervention possible.
Active Suicidal Ideation
If someone is experiencing active suicidal ideation, they are more likely to have answers for the questions about these various components. Active SI means that, in some sense, you are having active thoughts about suicide. This might mean that you are thinking about how you would kill yourself (plan) but don’t have a time frame or intent. Maybe you have a plan of how you would kill yourself and access to means, but the severity is low. There is any number of combinations for the SI factors that you’re experiencing.
Someone with imminent risk for suicide typically has a plan, access to the means to follow through with their plan, a time frame, and the intent to follow through. This is a severe experience of SI. This severity level might require a more involved intervention to protect your safety. Interventions appropriate for imminent risk for suicide might involve friends and family in safety planning, considering an intensive outpatient program, or psychiatric hospitalization.
Passive Suicidal Ideation
Passive suicidal ideation is suicidal ideation without a plan. If you asked the questions above, you might get a response like, “I’m not sure; I just wish that I were dead.”
Some additional ways that passive suicidal ideation may be communicated are:
I wish I had never been born.
I would be okay if I didn’t wake up tomorrow.
Everyone is worse off with me in their lives.
Sometimes when I’m driving, I hope there’s an accident, and I don’t survive.
Passive SI does not include active thoughts about suicide, but it is still important to identify and take it seriously. It frequently comes from a place of dealing with anxiety and depression or feeling hopeless about a situation or symptoms. People who are experiencing passive suicidal ideation also need support and care. Dismissing someone’s passive SI is very reductive and will most likely lead to them feeling more alone.
If you are worried that someone you care about might be suicidal, ask them. The best way to support someone who is dealing with suicidal ideation is to have an honest conversation about it. This is the best starting place to identify what’s going on, what coping skills might help, and what support they need.
If you or someone you care about is experiencing suicidal ideation and needs therapeutic support, sign up for a free 30-minute consultation with our therapist matchmaker to find the therapist who’s your best therapeutic match.
All therapists at Woven Together Trauma Therapy are trauma-informed and specialize in treating all forms of trauma. We also offer EMDR Therapy, Ketamine Assisted Psychotherapy, and Brainspotting Therapy which have shown to be extremely effective in treating and healing treatment-resistant depression as well as helping with suicidal ideation. Want to read more about our unique therapy options?
These blogs talk more about the basics of EMDR Therapy:
You can read more about Ketamine Assisted Psychotherapy here:
If you would like to learn more about Brainspotting Therapy, check out our blog: What is Brainspotting?
Learn More About Our Approach To Therapy





























